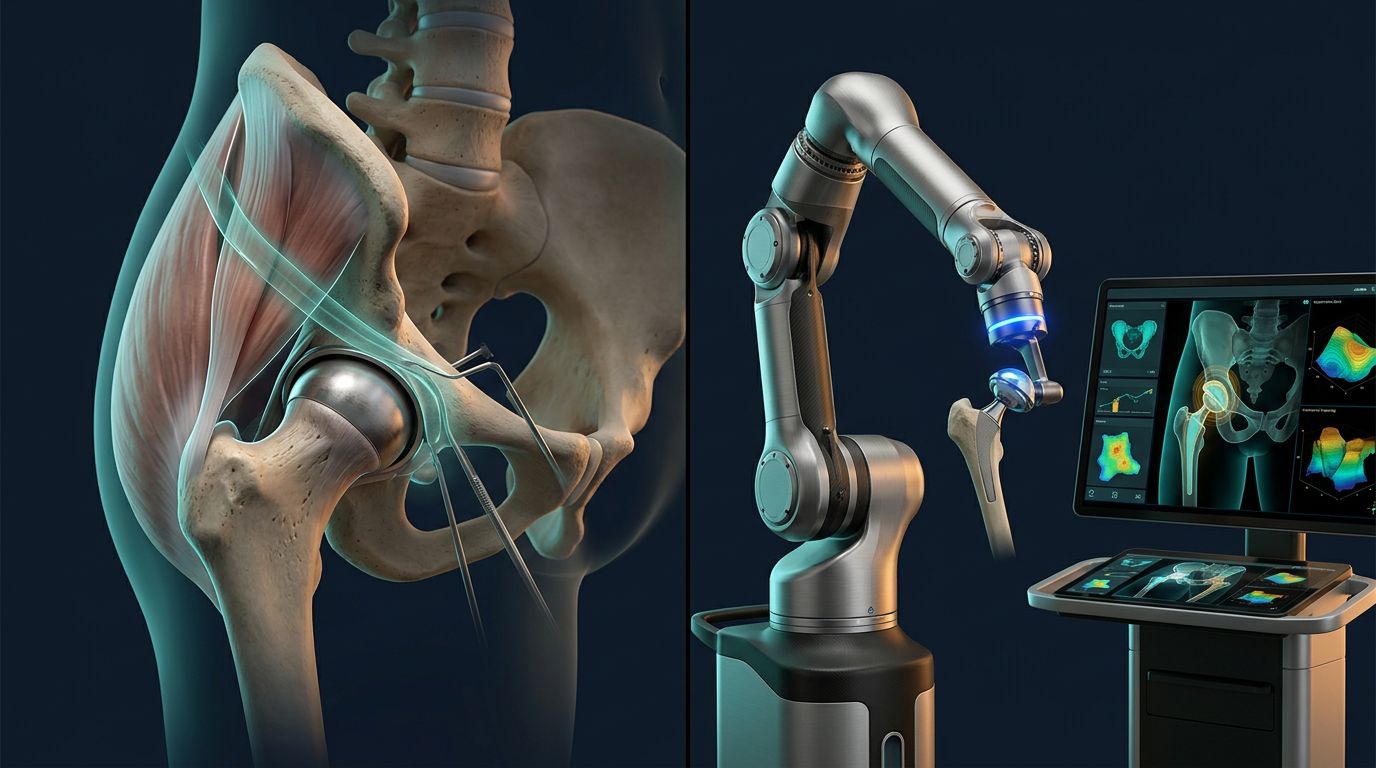
Hip replacement has changed, but the terminology can still be confusing. When you compare SuperPATH vs robotic hip surgery , you're comparing two different features of a procedure: one describes the surgical approach, while the other describes technology used to plan and guide...

Avascular necrosis can damage the hip silently until bone collapse causes severe pain and stiffness. For some patients with advanced disease, SuperPATH hip replacement offers a tissue-sparing approach to replacing the damaged joint. The right treatment depends on the stage of...

At 80, severe hip pain can make ordinary activities feel out of reach. Walking across the room, getting dressed, or standing from a chair may become difficult. That often leads patients and caregivers to ask whether SuperPATH hip replacement is still an option. In many cases,...